
"How many grafts do I need?" It's the single most common question hair transplant patients ask — and the answer shapes everything from your budget to your technique options to whether your result looks life-changing or disappointing.The problem? Most online resources hand you a single number when what you actually need is a range tailored to your specific hair loss pattern, anatomy, and goals.
The average hair transplant involves between 2,500 and 4,500 grafts. That range is so wide it's nearly meaningless without context. A patient with mild temple recession and one with extensive crown loss have fundamentally different needs. A "one-size-fits-all" graft estimate is one of the biggest red flags in the hair transplant industry.
This guide changes that. Using the Norwood-Hamilton Scale — the internationally recognized classification system for male pattern baldness — we break down hair transplant grafts by Norwood stage, explain the personal factors that shift your number up or down, and give you the knowledge to evaluate any clinic's recommendation with confidence. By the end, you'll understand what your stage typically requires, why two patients at the same stage might need different graft counts, and how to take the next step toward a personalized plan.
Whether you've already received a quote and want to cross-reference it, or you're just beginning to explore your options, this guide covers everything:
- Graft ranges for every Norwood stage (2 through 7)
- What 3,000, 4,000, and 5,000 grafts can realistically achieve
- The personal factors that shift your graft count up or down
- How to evaluate a clinic's estimate and spot red flags
- Donor supply limits, session planning, and cost considerations
You can also get your personalized graft estimate using our online calculator for a quick starting point.
This article is for informational purposes only and does not constitute medical advice. Only a qualified surgeon can determine your exact graft count after a thorough examination. Individual results vary based on personal anatomy, health, and other factors.
Grafts vs. Hairs — Why This Distinction Matters
Before the graft ranges in this guide mean anything, you need to understand the unit of measurement. It's the single most common source of confusion in hair transplant planning — and some clinics exploit it deliberately.
What Is a Graft?
A graft, also called a follicular unit, is a naturally occurring cluster of 1–4 hair follicles that grow together as a group. Think of it as a tiny bundle rather than a single strand. When a surgeon extracts and transplants hair, they work with these natural groupings to produce realistic-looking results.
On average, each graft contains approximately 2.2 hairs, though this varies by ethnicity and individual genetics. Some grafts contain just a single hair — these are often placed along the very front of the hairline for a natural, feathered edge. Others contain 3 or 4 hairs and deliver more density per unit.
This means 3,000 grafts translates to roughly 6,000–6,600 individual hairs. That's significant coverage from what might sound like a modest number
Why Clinics Count in Grafts, Not Hairs
Grafts are the standardized unit of extraction and implantation across the hair transplant industry. Every reputable clinic quotes procedures in grafts because that's what the surgeon physically removes and places.
However, some clinics advertise in "hairs" rather than grafts. This makes their numbers sound dramatically larger — a 3,000-graft procedure suddenly becomes "6,600 hairs." If a clinic emphasizes hair count over graft count, treat it as a red flag. It's often a marketing tactic designed to make the procedure sound more impressive than a competitor's equivalent offer.
How Graft Count Translates to Visual Density
Not all grafts create the same visual impact. In clinical practice, surgeons typically aim for 25–35 grafts per cm² across most of the scalp. For the hairline zone — where density and naturalness matter most — the target increases to 40–50 grafts per cm².
The relationship between graft count and perceived fullness isn't purely mathematical, though. Hair thickness, color, texture, and curl pattern all influence how "full" a given number of grafts will look. These variables can shift your personal graft count significantly — and we'll explore each one in detail later.
Understanding the Norwood Scale — Where Do You Fall?
Now that you understand the unit of measurement, the next step is identifying your level of hair loss. The tool surgeons use worldwide for this is the Norwood-Hamilton Scale, commonly called the Norwood Scale.
The Norwood Scale classifies male pattern baldness into seven stages, from Stage 1 (no significant hair loss) to Stage 7 (the most extensive loss, with only a narrow band of hair remaining around the sides and back). Each stage describes a specific pattern of recession and thinning — and each corresponds to a general range of grafts needed for restoration.
In clinical practice, the majority of hair transplant patients fall between Norwood 3 and Norwood 5 when they first seek treatment — though patients at every stage from 2 to 7 are regularly treated. You can self-assess your stage by comparing your hair loss pattern to the descriptions below. However, professional evaluation is always more accurate. Photos can be misleading, and a trained surgeon can identify thinning that isn't obvious to the naked eye.
For a deeper dive into each stage, you can learn more about the Norwood Scale in our dedicated guide.
A brief note: the Norwood Scale applies to male pattern baldness. Female hair loss follows different patterns and is classified using the Ludwig Scale.
Understanding where you fall on the scale is the foundation for estimating how many grafts you need. The next section breaks this down stage by stage.
How Many Grafts Do I Need by Norwood Stage?
The following breakdown of hair transplant grafts by Norwood stage is based on clinical averages from thousands of procedures. These ranges represent what most patients typically require for meaningful, natural-looking restoration. Individual needs vary based on personal anatomy and goals — a point we'll reinforce throughout, because it cannot be overstated.
Each stage below covers the typical loss pattern, the specific scalp zones that need coverage, and the graft range you can expect.
Norwood 2 — Slight Recession at the Temples
At Norwood 2, hair loss is minimal. You'll notice a slight recession at the temples, creating a more "mature" hairline compared to the rounded, juvenile hairline of adolescence. The temporal peaks — the corners of the hairline — show the earliest signs of pulling back.
Zones affected: Frontal hairline corners (temporal peaks)
Graft range: 800–1,500 grafts
This is typically a single-zone procedure focused on hairline refinement rather than large-scale restoration. The goal is to restore the temporal angles and create a clean, defined frame for the face. These are estimates based on clinical averages, and your specific anatomy may shift this number in either direction.
One important planning consideration: some surgeons recommend waiting at Norwood 2 if the patient is young and hair loss is likely to progress. Others support early intervention for the psychological benefit and the advantage of working with a strong donor area. Opinions vary among surgeons, but the general consensus is that a conservative approach — one that leaves room for future procedures — is the safest strategy.
In practice, 1,000–1,500 grafts at this stage produces a subtle but noticeable improvement: a sharper, more youthful hairline that looks completely natural.
Norwood 3 — Noticeable Hairline Recession
Norwood 3 represents a clear progression. The temples have receded further, creating a distinct M-shape. In some patients, this stage includes early thinning at the crown (classified as Norwood 3 Vertex, or 3V), which changes the treatment plan.
Zones affected: Frontal hairline, temples, and possibly early crown thinning
Graft range: 1,500–2,500 grafts
Patients often ask how many grafts they need for Norwood 3, and the answer typically falls within this range. This is one of the most common stages for first-time hair transplant patients. The hair loss is noticeable enough to motivate action but not so advanced that donor supply is a concern.
The distinction between Norwood 3 and 3 Vertex matters. If the crown is also thinning, the graft count moves toward the higher end of the range — or the surgeon may recommend addressing the crown in a future session.
What we typically see at this stage is that 2,000 grafts provides strong frontal coverage with a natural, well-defined hairline. Patients often describe the result as "turning back the clock" by several years. Individual results vary based on hair characteristics, but Norwood 3 patients are generally excellent candidates for a single-session procedure with high-impact results.
Norwood 4 — Significant Frontal and Crown Loss
At Norwood 4, hair loss becomes more substantial. There's clear recession across the frontal zone, and the crown has developed a distinct thinning or bald spot. A bridge of hair may still separate the two areas, but it's often thinner than it appears.
Zones affected: Frontal zone, mid-scalp, and crown
Graft range: 2,500–3,500 grafts
This is where multi-zone planning becomes critical. Most experienced surgeons prioritize the frontal zone because it delivers tThis is where multi-zone planning becomes critical. Most experienced surgeons prioritize the frontal zone because it delivers the greatest visual impact — it's what you and others see first. he greatest visual impact — it's what you and others see first. The crown is typically addressed second, either within the same session or in a follow-up procedure.
The 3,000-graft procedure is one of the most commonly performed graft counts in hair transplantation, and Norwood 4 is a major reason why. It's a versatile number that allows comprehensive frontal restoration with meaningful crown coverage.
Based on the procedures we perform daily, 3,000 grafts at this stage typically delivers a result patients describe as transformative — a full-looking frontal zone with improved density across the mid-scalp. As with all stages, your individual anatomy and goals determine where you fall within this range.
It's important to set realistic expectations, though. Achieving maximum density in both the frontal zone and the crown within a single session may require prioritization. Your surgeon should walk you through the trade-offs before you decide.
Norwood 5 — Extensive Hair Loss
Norwood 5 marks a significant escalation. The bridge of hair between the frontal zone and the crown has thinned dramatically or disappeared entirely. The bald area now covers a large portion of the top of the scalp.
Zones affected: Full frontal zone, mid-scalp, and crown
Graft range: 3,500–5,000 grafts
Donor supply becomes a more pressing consideration at this stage. The average scalp donor area yields 6,000–8,000 extractable grafts over a lifetime, and a Norwood 5 patient may need a significant portion of that supply in a single procedure.
The honest answer is that full coverage is achievable for most Norwood 5 patients, but ultra-high density across all three zones may not be realistic in one session. Some patients opt for a strategic approach: high density in the frontal zone and moderate density in the crown, with the option for a second session later to increase overall fullness.
Patients asking specifically about how many grafts for the crown area can typically expect 800–1,500 grafts dedicated to the crown alone, depending on the size of the thinning zone. The remaining grafts cover the frontal and mid-scalp regions.
In practice, 4,000 grafts at Norwood 5 delivers a dramatic improvement — a restored hairline, filled mid-scalp, and visible crown coverage. Patients go from an obviously thinning appearance to one that looks naturally full, though individual results depend on hair caliber, color contrast, and other factors covered below.
Norwood 6 — Advanced Hair Loss
At Norwood 6, only a horseshoe-shaped band of hair remains on the sides and back of the head. The
Zones affected: Entire top of the scalp from hairline to crown
Graft range: 5,000–6,500 grafts
Donor supply is now the primary limiting factor. Here's what most articles won't tell you: achieving full, youthful density across the entire scalp at Norwood 6 may require two sessions — and in some cases, it may not be fully possible regardless of session count. Any clinic that promises otherwise should be approached with caution.
Strategic planning is essential. Most surgeons focus on creating the strongest possible frontal zone and mid-scalp coverage first, as these areas have the most dramatic impact on overall appearance. The crown receives moderate density to eliminate the obviously bald look.
For patients with strong donor characteristics, body hair transplant (BHT) — using beard or chest hair as a supplementary donor source — may be discussed. This isn't standard practice for every patient, but it can extend the available graft supply in select cases.
A 5,000-graft procedure at Norwood 6 typically produces a meaningful, natural-looking improvement that significantly changes the patient's appearance. The goal shifts from "restoring every hair" to "creating the most impactful result with the resources available."
Norwood 7 — Maximum Hair Loss
Norwood 7 represents the most extensive pattern of male hair loss. Only a narrow band of donor hair remains, and the area requiring coverage spans the entire scalp surface.
Zones affected:Entire scalp surface
Graft range: 6,000–8,000+ grafts (often across multiple sessions)
Not every patient is a candidate for transplantation at this stage. Candidacy assessment is critical — the surgeon must evaluate whether the remaining donor area can supply enough grafts to create a result that looks natural and worthwhile. A professional assessment from an experienced surgeon is essential before proceeding.
The goal at Norwood 7 shifts from "a full head of hair" to "meaningful, natural-looking improvement." Multi-session planning is almost always necessary, with sessions spaced 9–12 months apart to allow full healing and growth.
The importance of choosing a surgeon who will be honest about what's achievable cannot be overstated. In our experience, the patients most satisfied at this stage are those whose surgeon set clear, realistic expectations from the beginning — not those who were promised the most grafts.
The following table summarizes the graft ranges, zones, and session expectations for each Norwood stage:
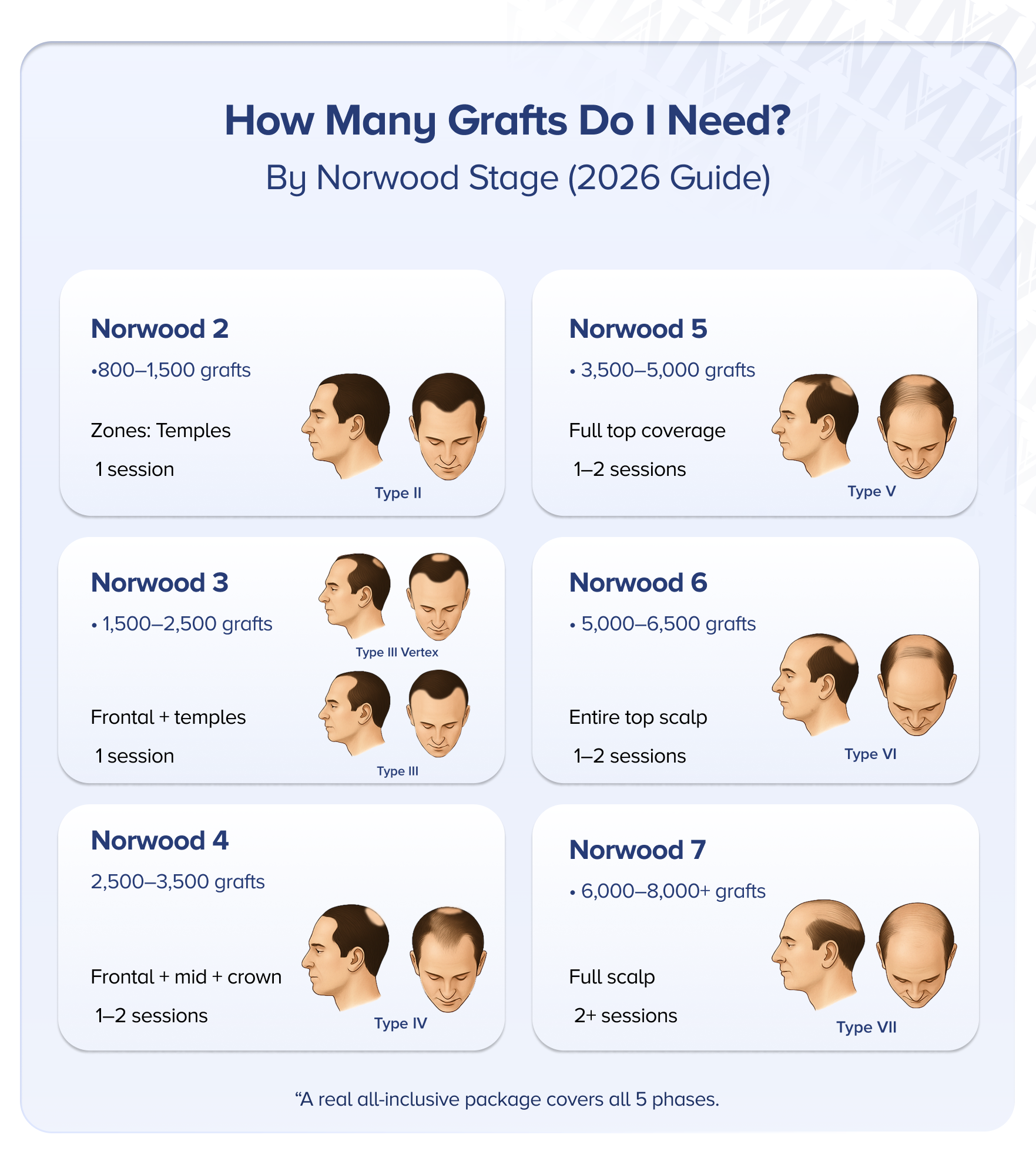
| Norwood Stage | Graft Range | Primary Zones | Typical Sessions |
|---|---|---|---|
| Norwood 2 | 800–1,500 | Temporal peaks, frontal hairline | 1 session |
| Norwood 3 | 1,500–2,500 | Frontal hairline, temples, early crown (3V) | 1 session |
| Norwood 4 | 2,500–3,500 | Frontal zone, mid-scalp, crown | 1 session (occasionally 2) |
| Norwood 5 | 3,500–5,000 | Full frontal, mid-scalp, crown | 1–2 sessions |
| Norwood 6 | 5,000–6,500 | Entire top of scalp | 1–2 sessions |
| Norwood 7 | 6,000–8,000+ | Entire scalp surface | 2+ sessions |
All ranges are clinical averages. Individual needs vary based on anatomy, hair characteristics, and personal goals. Only a personalized consultation can determine your exact number.
Want to see what these graft counts look like in real life? View our patient gallery to browse results from patients at every Norwood stage.

What About 3,000 Grafts, 4,000 Grafts, or 5,000 Grafts Specifically?
Understanding your Norwood stage gives you a baseline — but many patients approach the question from the opposite direction. They've received a specific graft count in a quote and want to know what that number can actually deliver.
What Can 3,000 Grafts Achieve?
A 3,000 grafts hair transplant is one of the most common and versatile procedures performed. It's typically ideal for Norwood 3–4 patients and translates to approximately 6,000–6,600 individual hairs.
At this graft count, expect comprehensive coverage of the frontal zone and mid-scalp with good density. For a Norwood 3 patient, 3,000 grafts often provides a surplus that allows higher-density packing in the hairline. For a Norwood 4 patient, it covers the frontal zone thoroughly with moderate crown improvement.
Is 3,000 grafts enough for a hair transplant? For mild to moderate hair loss, it's often more than sufficient. For extensive loss (Norwood 5+), it typically falls short of full coverage.
What Can 4,000 Grafts Achieve?
A 4,000 grafts hair transplant suits Norwood 4–5 patients and provides approximately 8,000–8,800 hairs. This count allows coverage of the frontal zone, mid-scalp, and partial crown — or comprehensive frontal coverage with higher-density packing along the hairline.
The additional 1,000 grafts over a 3,000-graft procedure provides meaningful flexibility. Surgeons can distribute them strategically, adding density where it matters most for your specific pattern. Session duration increases accordingly, typically running 6–8 hours or longer depending on the technique and team size.
What Can 5,000 Grafts Achieve?
A 5,000 grafts hair transplant is appropriate for Norwood 5–6 patients and delivers approximately 10,000–11,000 hairs. This is a comprehensive procedure covering multiple zones with meaningful density across the entire treatment area.
A procedure of this size requires strong donor supply. Your surgeon must verify that your donor area can sustain this level of extraction without visible thinning. In some cases, 5,000 grafts pushes the limits of a single session — most reputable clinics cap single-session FUE at 4,500–5,500 grafts.
Mega-sessions — large single-day procedures — are possible with experienced teams, but the surgeon's skill and the clinic's infrastructure matter enormously at this volume. To understand what 5,000 grafts before and after looks like in practice, patient galleries offer the most realistic reference point.
7 Factors That Affect How Many Grafts You Need
Your Norwood stage provides a starting range — but several personal factors can shift that number considerably. Two patients at the same Norwood stage can receive very different graft estimates. Understanding these variables empowers you to make sense of your number and ask the right questions.
1. Hair Caliber (Thickness)
Hair caliber refers to the diameter of each individual hair strand. Thicker hair provides substantially more coverage per graft because each strand occupies more visual space. Think of it like painting with a broad brush versus a fine-tipped pen — fewer strokes cover the same area.
Patients with fine hair may need more grafts to achieve the same perceived density as someone with coarse, thick hair. This is one of the most significant variables in graft planning.
2. Donor Area Density
Your donor area — the band of hair on the sides and back of your head that resists pattern baldness — has a finite number of available grafts. Higher donor density means more grafts can be extracted without visibly thinning the donor zone.
Average donor density is approximately 65–85 follicular units per cm². Patients at the higher end have more flexibility in planning. Those at the lower end may need a more conservative approach to preserve the donor area's natural appearance.
3. Hair-to-Skin Color Contrast
This factor is often overlooked but has a dramatic impact on perceived density. Low contrast — such as blonde hair on fair skin or dark hair on dark skin — creates a natural illusion of greater fullness. High contrast — such as jet-black hair on very pale skin — makes every gap between hairs more visible, requiring more grafts for the same visual result.
4. Hair Texture (Straight vs. Curly)
Curly and wavy hair provides significantly more ground coverage per graft than straight hair. Each curl creates volume and overlap that fills space more effectively. Picture the difference between laying coiled springs versus straight pins across a surface — the coils cover far more area.
In clinical practice, patients with straight, fine hair typically need more grafts than those with curly or wavy hair to achieve comparable fullness.
5. Scalp Laxity
Scalp laxity — how loose or tight the skin on your scalp is — affects how many grafts can be safely extracted in a single session. Tighter scalps make extraction more difficult and may limit the total graft count per procedure. Your surgeon assesses this during the consultation by gently manipulating the scalp to gauge its flexibility.
6. Desired Density and Hairline Design
Your personal goals play a significant role. A patient who wants a conservative, age-appropriate hairline needs fewer grafts than someone requesting a more aggressive, lower hairline. Similarly, prioritizing maximum density in the frontal zone over crown coverage changes the distribution plan entirely.
This is where the conversation between you and your surgeon matters most. The right questions to ask are: "What hairline design do you recommend for my age and face shape?" and "How will you distribute grafts across the zones?"
7. Future Hair Loss Progression
This is especially critical for younger patients. Hair loss is progressive — the pattern you have today may not be the pattern you have in five or ten years. Surgeons must plan for continued loss, particularly in patients under 25 whose hair loss patterns may not be fully established.
Consider a 28-year-old Norwood 3 patient who wants an aggressive, low hairline using maximum grafts. A conservative approach — transplanting fewer grafts now and preserving donor supply for future sessions — is almost always the smarter long-term strategy. Using all available grafts today leaves nothing in reserve if hair loss continues. And it very likely will.
Medical treatments such as finasteride or minoxidil may help slow further loss and complement surgical results — discuss these options with your doctor.
Key takeaway: Imagine two Norwood 4 patients who both receive 3,500 grafts. Patient A has thick, dark, curly hair on olive skin. Patient B has fine, straight, black hair on very pale skin. Patient A's result looks dramatically fuller — each graft provides more visual coverage and lower contrast hides gaps. Same graft count, strikingly different outcomes. This is why graft count alone never tells the full story.
Quick Quote in 5 Minutes
Talk to an experienced patient coordinator for your hair transplant in Turkey.How Surgeons Determine Your Graft Count
At this point, you might be wondering: how does a surgeon arrive at a specific number for my situation? The process is more detailed than many patients expect — and understanding it helps you evaluate any clinic's proposal.
The consultation typically begins with a review of your medical history, including the timeline of your hair loss, any medications you're taking, and family history of baldness. From there, the surgeon moves to a physical scalp analysis using several tools:
- Densitometry — a magnification device that measures the number of follicles per square centimeter in your donor area
- Digital photography — for zone-by-zone mapping and documentation
- Manual scalp assessment — evaluating hair caliber, scalp laxity, and donor density by touch
- Recipient area measurement — calculating the total surface area requiring coverage
Based on this data, the surgeon creates a zone-by-zone plan. Rather than assigning a single number to your entire head, they allocate specific graft counts to each zone: a set number for the frontal hairline, a set number for the mid-scalp, and a set number for the crown. This ensures strategic distribution rather than uniform spreading.
Your goals and expectations factor into the final plan as well. A patient who prioritizes a dense hairline receives a different distribution than one who wants balanced coverage everywhere.
Why two clinics might give different estimates: Varying graft counts from different clinics are common. Imagine you consult three clinics — one quotes 2,500 grafts, another 3,200, and a third 4,500. The first may be conservative, the second balanced, and the third may be inflating numbers. A difference of 500 grafts is normal and reflects different surgical philosophies. A difference of 2,000 grafts warrants scrutiny — ask each clinic to explain their zone-by-zone rationale. At Medart Hair, every patient receives a detailed scalp analysis and zone-by-zone graft plan because transparent planning is the foundation of a successful procedure.
Armed with this information, you can evaluate any clinic's proposal critically. Ask for a breakdown by zone. Ask why they chose that number. The answers will tell you a great deal about the clinic's integrity
Do I Have Enough Donor Hair? Understanding Donor Supply Limits
One of the most important — and most overlooked — aspects of hair transplant planning is donor supply. Your donor area is not an unlimited resource. Think of it like a bank account with a fixed balance: you can make withdrawals, but once the funds are depleted, they don't replenish.
The average person has approximately 6,000–8,000 extractable grafts in the scalp donor zone. This is a lifetime total — it includes all current and future procedures combined. For patients at Norwood 2–4, this supply is typically more than sufficient. For Norwood 6–7 patients, demand may approach or exceed supply.
Over-harvesting — extracting too many grafts from the donor area — creates serious problems:
- Visible thinning in the donor zone that's difficult to conceal
- A moth-eaten or patchy appearance at the back and sides of the head
- Scarring that limits options for future proceduresh
- Compromised results if grafts are extracted from weaker follicles at the zone's edges
Ethical clinics will tell you if your expectations exceed your donor capacity — rather than extracting aggressively to hit a promised number.
This is where donor management becomes essential. A responsible surgeon plans not just for today's procedure but for potential future sessions. If you're 35 with Norwood 4 hair loss, your surgeon should consider that you may need additional grafts at 45 or 50 as hair loss progresses.
For patients with limited scalp donor supply, alternative sources exist. Beard and chest hair can serve as supplementary donors in select cases. However, body hair differs in texture and growth cycle from scalp hair, so it's typically used to add density in less visible areas rather than to construct a hairline.
Before any procedure, ask your surgeon to show you the donor density assessment and explain how many grafts can be safely extracted while maintaining a natural-looking donor area. Any clinic that promises unlimited grafts without discussing donor limitations is not being honest with you.
One Session or Two? When Multiple Procedures Are Needed
Knowing your graft range naturally raises the next question: can all of those grafts be transplanted in a single session?
Most reputable clinics cap single-session FUE procedures at 4,500–5,500 grafts. This isn't an arbitrary limit — it's rooted in biology. Each graft spends time outside the body between extraction and implantation. The longer that window, the lower the survival rate. Well-performed FUE achieves 90–95% graft survival, but pushing beyond safe session limits can compromise this significantly.
Patients needing 5,000+ grafts — typically Norwood 5 and above — often benefit from splitting the procedure into two sessions. Two sessions are generally recommended when:
- The total graft count exceeds 5,000–5,500
- The patient wants ultra-high density across multiple zones
- Donor area characteristics limit safe extraction in a single sitting
- The patient prefers a more gradual, staged approach
The typical timeline between sessions is 9–12 months. This allows transplanted grafts to fully establish and grow, giving the surgeon a clear picture of first-session results before planning the second.
If you're wondering about how many hair transplants you can have over your lifetime, the answer depends primarily on your donor supply. Most patients can safely undergo 2–3 procedures, provided each session is planned conservatively.
For patients traveling to Turkey, multi-session planning requires additional logistical consideration — travel, accommodation, and time off work for each trip. Many clinics in Istanbul offer all-inclusive packages that simplify this, covering accommodation and transfers alongside the medical procedure.
Does Hair Transplant Technique Affect Graft Count?
You've likely encountered several technique names in your research — FUE, Sapphire FUE, DHI — and you may be wondering whether your choice of method changes how many grafts you need. The short answer: it doesn't. Your anatomy and hair loss pattern determine that number regardless of technique.
Here's how the three main methods differ in practice:
- FUE (Follicular Unit Extraction) is the foundational method. Individual grafts are extracted from the donor area using a micro-punch tool and implanted into pre-made incisions in the recipient area.
- Sapphire FUE uses blades made from sapphire crystal to create the recipient incisions. These finer incisions allow closer graft placement, which can enable higher density in certain zones, depending on the surgeon's expertise.
- DHI (Direct Hair Implantation) uses a specialized pen (Choi pen) that simultaneously creates the incision and places the graft. This can achieve precise density in targeted zones and is particularly effective for hairline work.
What technique does affect is how grafts are placed and at what density per session. Sapphire FUE may allow slightly more grafts per cm² than standard FUE in certain cases. DHI sessions may take longer per graft, which can limit the total count achievable in a single session.
The clinical consensus is clear: the surgeon's skill and experience matter far more than the technique name on the brochure. Avoid choosing a clinic based solely on technique marketing. Evaluate the surgeon's track record, their approach to your specific case, and the quality of their results.
How Graft Count Affects Hair Transplant Cost
Graft count and cost are inextricably linked — it's one of the first calculations every patient makes. Understanding how pricing works helps you budget accurately and avoid overpaying.
Most clinics use a per-graft pricing model, where you pay a set rate multiplied by the number of grafts transplanted. Your total cost scales directly with your graft count. For a detailed explanation of how this model works, see our cost per graft page
Turkey offers significantly lower per-graft costs compared to the UK, US, or Western Europe — often a fraction of the price for equivalent quality. This cost difference is driven by lower overhead and operating costs, not by lower standards of care. However, the cheapest per-graft price isn't always the best value.
When evaluating cost, consider the full picture:
- Surgeon experience and credentials — who is actually performing the procedure?
- Technique and technology — what tools and methods are being used?
- Aftercare and follow-up — what support do you receive after the procedure?
- All-inclusive packages vs. per-graft pricing — does the quoted price cover everything, or are there hidden costs?
A 3,000-graft procedure at a reputable clinic with an experienced surgeon is a better investment than a 5,000-graft procedure at a facility that cuts corners. For a comprehensive overview of what to expect financially, our hair transplant cost breakdown covers all the variables.
Common Mistakes When Estimating Graft Count
Even well-researched patients fall into predictable traps when planning their procedure. Recognizing these mistakes before your consultation can save you money, protect your donor area, and lead to a far better result.
Mistake 1: Confusing grafts with hairs. As covered earlier, a graft contains multiple hairs. If a clinic tells you they'll transplant "10,000 hairs," that's likely 4,000–4,500 grafts — a standard procedure, not the extraordinary number it sounds like. Always confirm whether a quote is in grafts or hairs.
Mistake 2: Fixating on a specific number without understanding your anatomy. Saying "I want 4,000 grafts" without knowing your Norwood stage, donor density, or hair caliber is like ordering a prescription without a diagnosis. The number should follow from the assessment, not the other way around.
Mistake 3: Choosing a clinic because they promised the highest graft count. This is one of the most dangerous mistakes. Clinics that promise significantly more grafts than competitors may be over-extracting from the donor area, using aggressive techniques that compromise graft survival, or simply inflating numbers to win your business. More grafts does not mean better results.
Mistake 4: Ignoring future hair loss. If you're under 40 and experiencing progressive hair loss, using your entire donor supply today leaves nothing for the future. A conservative, long-term strategy almost always produces better lifetime outcomes.
Mistake 5: Not considering donor supply limitations. Every graft extracted is one fewer graft available for future procedures. Patients who don't factor in their finite donor supply risk needing additional work they can't support.
Mistake 6: Comparing your graft count to someone else's. "My friend got 3,000 grafts and looks great — I should get 3,000 too." But your friend may have thicker hair, a different Norwood stage, curlier texture, or lower color contrast. Comparing graft counts without accounting for these variables leads to mismatched expectations every time.
Learn How Many Graft Do You Need?
Talk to an experienced patient coordinator for your hair transplant in Turkey.Frequently Asked Questions
Your Next Step: From Estimate to Personalized Plan
You now understand the graft ranges for each Norwood stage, the personal factors that shift those numbers, and the questions to ask any clinic that gives you an estimate. That puts you ahead of most patients walking into their first consultation.
But no guide — no matter how detailed — can replace a personalized assessment from an experienced surgeon. Your hair caliber, donor density, scalp laxity, and goals are unique to you. The ranges in this article give you a framework. The precise number requires hands-on evaluation.
There are two ways to take the next step:
- Get an instant estimate: Use our free graft calculator to receive a preliminary graft range based on your hair loss pattern. It takes less than a minute and gives you a solid starting point for further conversations.
- Get a personalized plan: Book a free consultation with our medical team for a detailed, zone-by-zone assessment. You'll receive an honest graft count based on your anatomy, a recommended technique, and a clear explanation of what results you can realistically expect. Initial assessments can be done remotely via photos, making the process straightforward for international patients.
Every patient who comes to us receives the same thing: a transparent plan built around what's achievable for them — not an inflated number designed to close a sale. That commitment to honest, individualized planning is the foundation of every procedure at Medart Hair.
