

Why Crown Hair Transplants Are More Challenging
The crown isn't just another zone on the scalp. It presents four distinct challenges that make it more technically demanding than hairline restoration — and understanding these will help you set realistic expectations and evaluate surgeons more effectively.
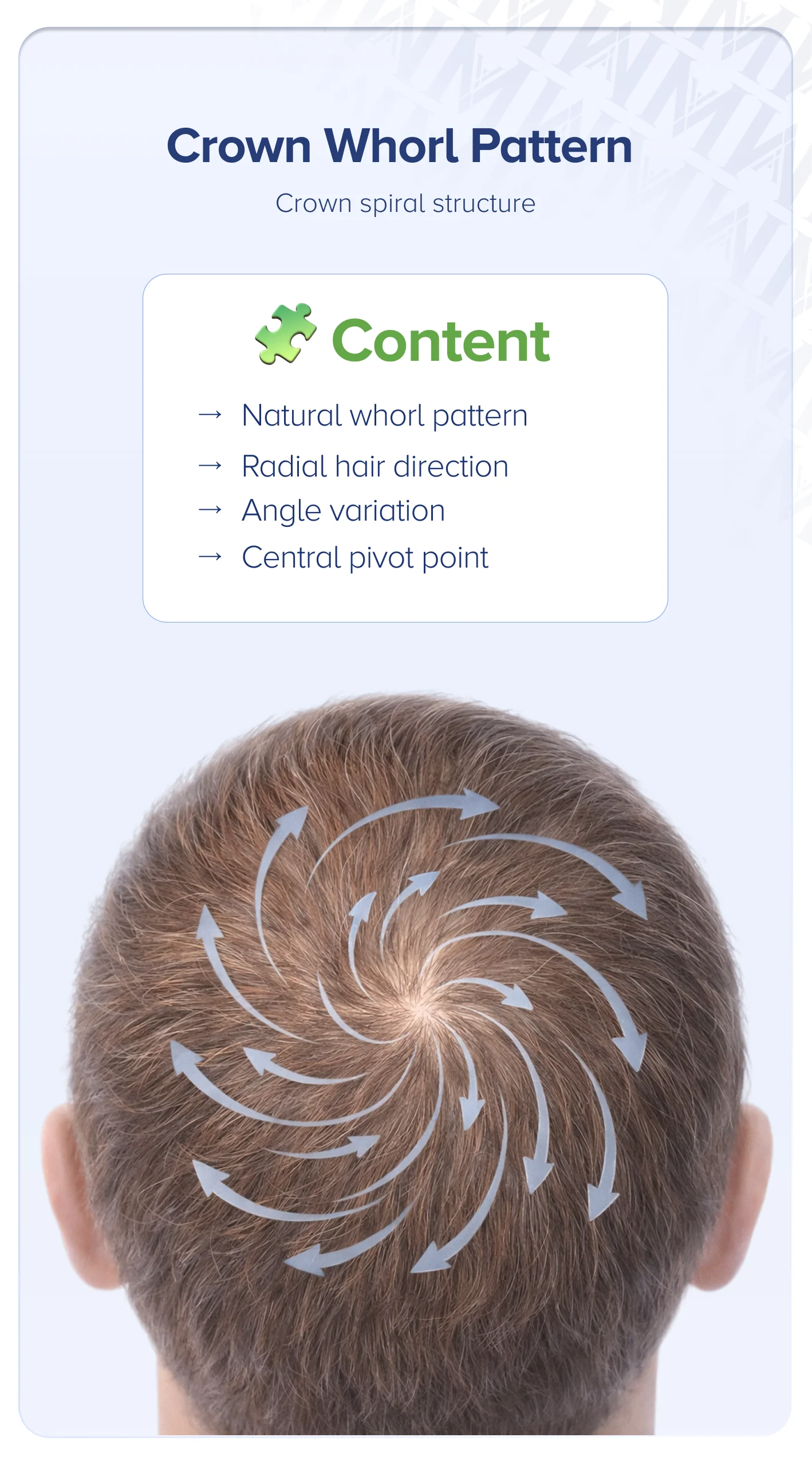
The Whorl Pattern Problem
At the hairline, grafts are placed in roughly parallel rows at a forward angle. The crown is fundamentally different. Here, the surgeon must replicate that natural spiral growth direction — placing each graft at a precise angle and orientation that radiates outward from the central whorl point.
Get this wrong, and the result looks flat, unnatural, or creates an awkward "starburst" effect where hairs stick up instead of lying smoothly. Whorl replication is one of the most demanding aspects of crown surgery, requiring meticulous pre-operative mapping and steady, experienced hands during graft placement. This is artistry as much as it is surgery.
Lower Blood Supply and Graft Survival
The scalp at the vertex has slightly lower blood supply (vascularity) compared to the frontal region. According to published clinical data, graft survival rates — the percentage of transplanted follicles that take root and grow — are generally reported at 85–92% at the crown, compared to 90–95% for frontal areas. The difference sounds small. Over hundreds or thousands of grafts, it adds up.
Experienced clinics mitigate this through careful graft handling, optimized recipient site density, post-operative protocols, and sometimes PRP (platelet-rich plasma) therapy. Some emerging evidence suggests PRP may support graft survival, though long-term data is still being established. The key takeaway: technique and clinic protocols matter more at the crown than almost anywhere else on the scalp.
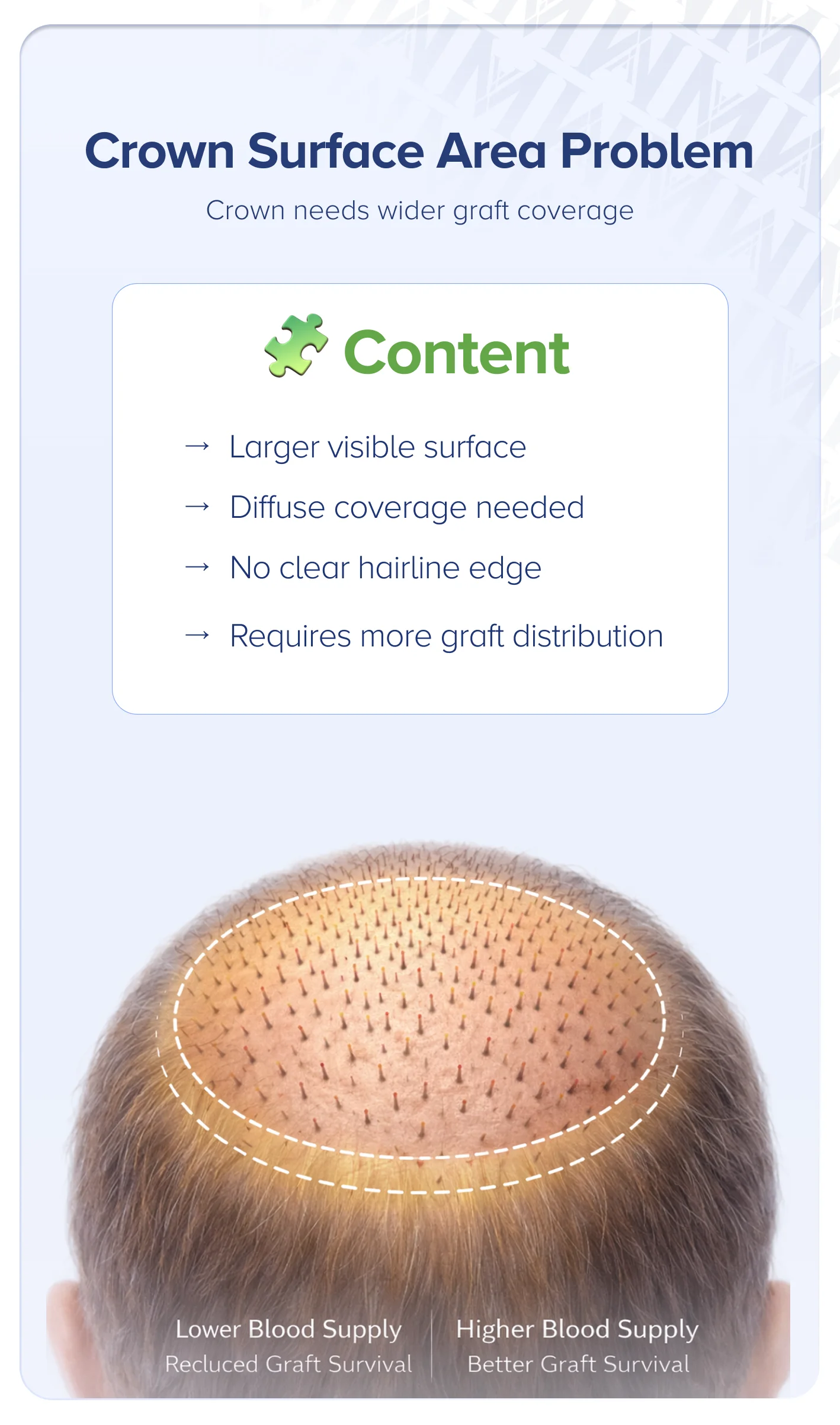
Larger Surface Area, Higher Graft Demand
Think of the difference between painting a flat wall and painting a dome. The crown is a convex surface, which means it has a larger visible area than it appears when measured flat. Depending on the degree of loss, the crown can span 80–120+ square centimeters.
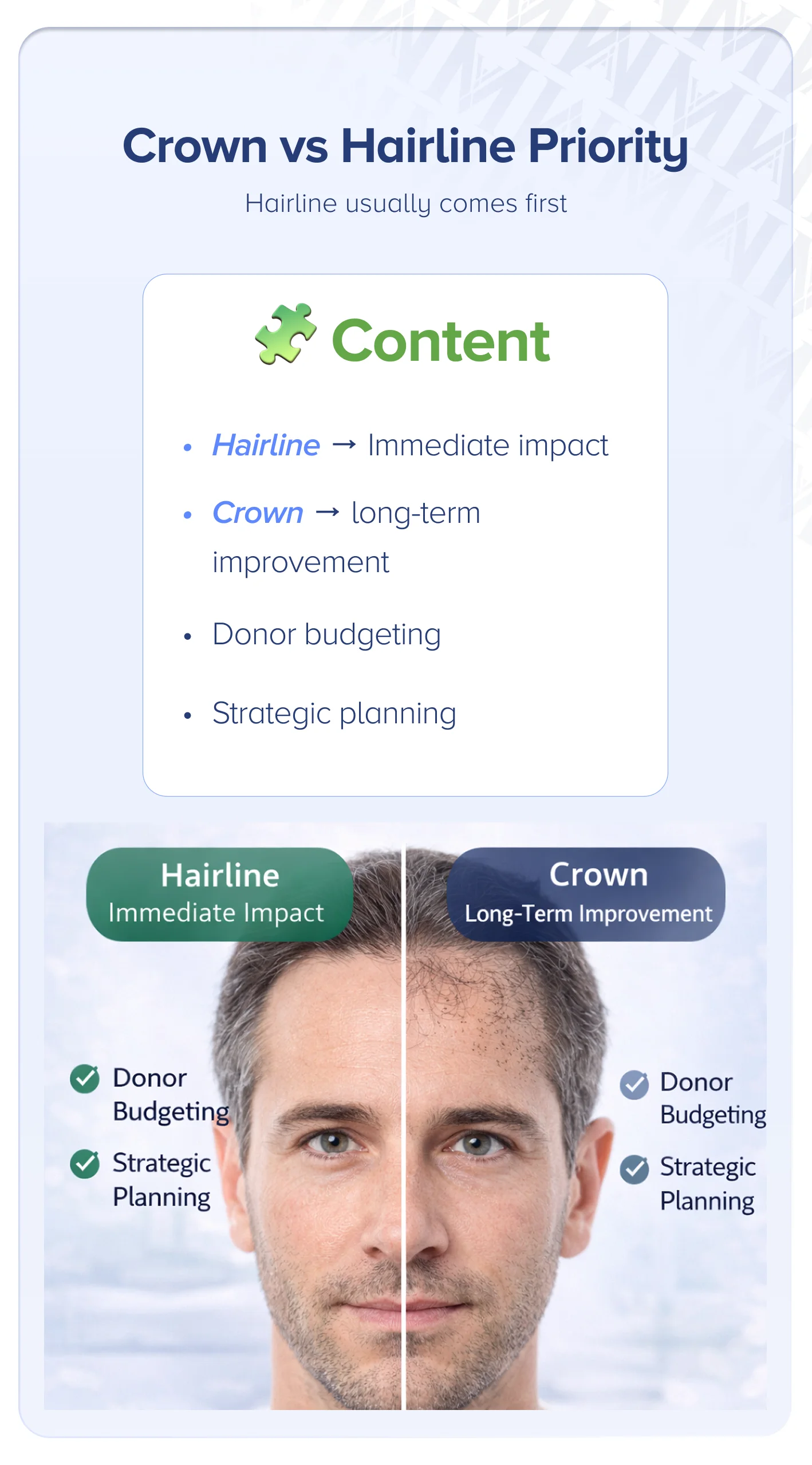
Unlike the hairline — where even one to two centimeters of dense coverage creates a dramatic visual frame — the crown demands broader, more diffuse coverage across this entire surface. There's no single "edge" to define. You need enough grafts distributed across the whole area to eliminate that visible bald spot, and that requires careful planning.

Ongoing Hair Loss — The Moving Target
This is arguably the most critical challenge. The crown is often the last area to stabilize in male pattern baldness. If you transplant grafts into the crown while the surrounding native hair is still thinning, you risk creating an "island" effect — a patch of transplanted hair surrounded by progressively thinner native hair that looks unnatural over time.
This is the primary reason many surgeons advise caution with crown transplants in younger patients, and why medication plays such a pivotal role in crown restoration strategy.
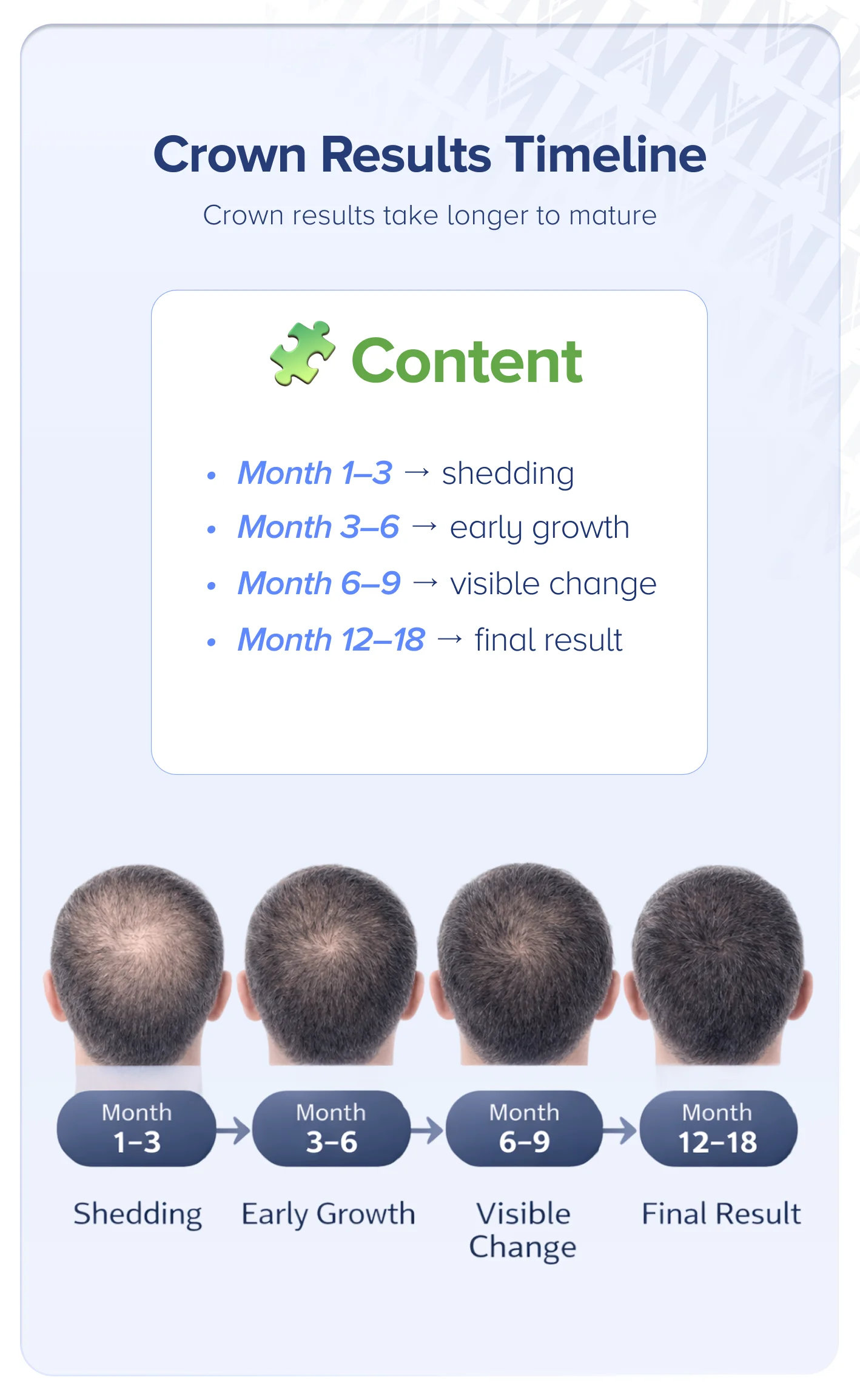
These challenges directly shape one of the most practical questions patients ask: how many grafts will the crown actually need?
Risks and Potential Complications Specific to Crown Transplants
Every surgical procedure carries risks. Crown transplants have specific concerns worth understanding before you commit. Individual outcomes vary based on genetics, health, surgeon skill, and post-operative care.
Lower Graft Survival Rate and How to Mitigate It
As discussed earlier, graft survival at the crown is generally reported at 85–92% in published clinical data — slightly lower than the 90–95% typical of frontal transplants. The lower blood supply at the vertex is the primary factor.
Experienced clinics minimize this gap through meticulous graft handling (keeping grafts hydrated and cool outside the body), optimized recipient site density (not overcrowding, which can compromise blood flow), and supportive treatments like PRP. When evaluating clinics, ask specifically about their crown graft survival protocols.
Unnatural Appearance from Poor Whorl Replication
When the natural spiral growth pattern isn't respected during graft placement, the result can look obviously artificial. Hairs may stick up at odd angles, create visible lines, or fail to lie flat and blend with surrounding hair.
This is why crown-specific experience matters. When evaluating a surgeon's work, ask to see crown-specific before-and-after photos — not just hairline results. A surgeon who produces beautiful hairlines may not have the same expertise with the vertex's unique demands.
The Island Effect from Progressive Hair Loss
If native hair continues thinning around your transplanted grafts, you can end up with an isolated patch of dense transplanted hair surrounded by bare or thin scalp. This looks unnatural and may require additional procedures to correct.
Prevention strategies include medication (to slow ongoing loss), conservative graft placement (leaving room to address future thinning), and a staged approach that monitors progression between sessions. Patients under 25 with active crown thinning should consult a specialist before committing to surgery, as their hair loss patterns may not yet be fully established.
Consider a second illustrative example. A 24-year-old with early Norwood 3 Vertex thinning wants to address his crown immediately. An experienced surgeon would typically recommend starting finasteride, monitoring for 12 months, and reassessing. In many cases, medication alone provides enough improvement to delay surgery — and when surgery does happen later, the loss pattern is stable enough for confident planning.

Donor Area Depletion
Large crown procedures require significant graft numbers. If you've already had a hairline procedure — or plan to have one — the total demand on your donor area can be substantial. Over-harvesting leads to visible thinning or scarring in the donor region.
For patients with extensive loss (Norwood 6–7), body hair transplant (BHT) — harvesting grafts from the chest or beard — can serve as a supplementary donor source. Body hair has different characteristics than scalp hair, and results vary. This option is worth discussing with your surgeon if donor supply is a concern.